High Blood Pressure Or TENSION
உயர் இரத்த அழுத்தம் (Hypertension) என்பது இரத்த அழுத்தத்தை உயரச் செய்கின்ற நாள்பட்ட மருத்துவ நிலையாகும். இது
உயர் இரத்த அழுத்தம் என்றும் அல்லது
ஹெச்டி ,
ஹெச்டிஎன் அல்லது
ஹெச்பிஎன் என்றும் சுருக்கமாக சொல்லப்படுகிறது. "ஹைபர்டென்ஷன்" (உயர் இரத்த அழுத்தம்) என்ற சொல், பொதுவாக, உடலமைப்பு முழுவதையும் பாதிக்கின்ற, தமனிவழி உயர் இரத்த அழுத்தம் என்பதையே குறிக்கிறது.
[1]
உயர் இரத்த அழுத்தத்தை
அடிப்படையானது (முதன்மையானது) என்றோ அல்லது
இரண்டாம் நிலையிலானது என்றோ பிரிக்கலாம். அடிப்படையான அல்லது முதன்மையான உயர் இரத்த அழுத்தம் என்பது அதிகரித்த இரத்த அழுத்தத்தை விளக்குவதற்கு மருத்துவக் காரணம் எதையும் கண்டுபிடிக்க இயலாததாகும். இது பொதுவானது. ஏறத்தாழ 90-95 சதவிகித உயர் இரத்த அழுத்த நிலைகள் அடிப்படையான உயர் இரத்தமேஇரண்டாம் நிலை உயர் இரத்தம் அழுத்தம் என்பது சிறுநீரக நோய் அல்லது கட்டிகள் (அட்ரினல் சுரப்பி கட்டி அல்லது ஃபியோகிராமிசட்டோமா) போன்ற மற்ற நிலைகளால் ஏற்படும் விளைவாகும் (
அதாவது இரண்டாம் நிலை).
நீடித்த உயர் இரத்த அழுத்தம் , இதயச் செயலிழப்பு மற்றும் தமனி அளவுக்கு அதிகமாக விரிவடைதல் ஆகியவற்றிற்கான அபாய காரணிகளுள் ஒன்றாக இருப்பதுடன், நாட்பட்ட சிறுநீரக செயலிழப்பிற்கும் காரணமாகிறது. தமனி இரத்த அழுத்தத்தில் ஏற்படும் மிதமான உயர்வு கூட குறுகிய ஆயுட்காலத்திற்கு வழிவகுக்கலாம். தமனி இரத்த அழுத்தம் 50 சதவிகிதம் அல்லது, அதற்கும் அதிகமாக இருக்கின்ற நிலை என்று வரையறுக்கப்பட்டுள்ள கடுமையான உயர் அழுத்தங்களில் உரிய முறையில் சிகிச்சை அளிக்கப்பட்டால் தவிர, வாழ்நாளின் கால அளவு சில வ்ருடங்களுக்கு மடடுமே. 115 mmHg இதய சுருங்கியக்க அழுத்தத்தில் தொடங்கி (இதயக் கீழறைகள் சுருங்கும்போது கார்டியாக் சுழற்சியின் முடிவிற்கு அருகாமையில் ஏற்படுகின்ற தமனிகளில் ஏற்படும் உச்சபட்ச அழுத்தம்) 75 mmHg (பொதுவாக 115/75 mmHg என்று எழுதப்படுவது) இதய விரிவியக்கத்தில் (தமனிகளில் குறைந்தபட்ச அழுத்தமாக உள்ள, இதயக் கீழறைகள் இரத்தத்தால் நிரப்பப்படும்போது கார்டியாக் சுழற்சியின் தொடக்கத்திற்கு அருகாமையில் உருவாவது) கார்டியோவாஸ்குலர் நோயின் (சிவிடி) அபாயம் ஒவ்வொரு 20/10 mmHg அதிகரிப்பிற்கும் அதிகரிக்கிறது
Yogic Practices
OM -CHANTING -JAPAM
PRANAYAMA
MEDITATION
YOGA NITHRA
Myocardial Infarction (Heart Attack)
Myocardial infarction, commonly referred to as a heart attack, occurs when one or more coronary arteries become suddenly blocked, resulting in heart muscle death.
Also Known As: Acute Myocardial Infarction, Heart Attack
Basic Facts
- Myocardial infarction, commonly referred to as a heart attack, occurs when one or more coronary arteries become suddenly blocked, resulting in heart muscle death.
- Typical symptoms of a myocardial infarction include chest pressure or pain, shortness of breath, profound sweating, nausea, vomiting, and/or fainting.
- Myocardial infarction results from coronary artery disease (CAD), which is an accumulation of plaque inside the coronary blood vessels.
- When one of these plaques rupture, a clot forms rapidly at the site and causes a sudden obstruction of blood flow in the coronary artery.
- Without immediate treatment, a myocardial infarction can cause permanent damage to the heart muscle and chaotic, abnormal heart beating. Both conditions can cause death.
- Because of the seriousness of a myocardial infarction, seeking immediate medical attention is very important.
A More Detailed Explanation
Myocardial infarction, also known as MI or heart attack, is a condition when one or more of the coronary arteries which supply oxygen-rich blood to the heart muscle become suddenly blocked, resulting in heart muscle death.
In general, blockages result from plaques made of cholesterol and fats building up in the coronary arteries. The accumulation of this plaque is known as coronary artery disease (CAD). In many cases, the accumulation of plaque is a gradual process and can produce symptoms of chest pain or pressure known as angina pectoris, or angina.
In contrast to this gradual accumulation of plaque, a myocardial infarction occurs when a plaque suddenly ruptures, causing a rapid accumulation of clotting factors at the rupture site. This results in a sudden obstruction of blood flow in the coronary artery. This sudden obstruction prevents any blood from reaching the heart muscle. Without this vital supply of oxygen-rich blood, the heart muscle begins to die. The longer the obstruction persists, the greater the amount of heart muscle that dies.
Myocardial infarction is a medical emergency . Without treatment, substantial portions of the heart can be permanently damaged, preventing efficient pumping of blood to the rest of the body, and resulting in congestive heart failure. In addition, a myocardial infarction can cause ventricular arrhythmias, or rapid and chaotic beating of the lower chambers of the heart. In many cases, ventricular arrhythmias can cause cardiac arrest, stopping blood flow to the body and brain. If that happens, brain damage and death can result within minutes.
Because of these serious and potential life-threatening complications of a myocardial infarction, seeking immediate medical attention is very important.
Symptoms
Myocardial infarction symptoms are typically sudden in nature, and often persist for more than 20 minutes. Occasionally, symptoms can ‘come and go.’ Typical symptoms include:
- Chest pain or pressure
- Chest tightness
- Chest pain, pressure, or tightness that extends from the chest to the neck, throat, jaw, shoulder and/or arm
- Chest discomfort just below the breastbone
- Chest burning, similar to heartburn or indigestion
- Shortness of breath
Because a myocardial infarction usually occurs without warning, it can cause severe anxiety. It can also cause other symptoms such as nausea, lightheadedness, fainting, or profuse sweating.
Many people having symptoms of a myocardial infarction are reluctant to seek medical attention because they think the pain they are feeling is due to something else, are afraid or unwilling to admit that the pain could represent something serious, or are reluctant to ‘cause a scene’ by calling an ambulance, going to the hospital, and then discovering it is a false alarm.
However, by delaying medical attention and treatment, patients are at much higher risk for permanent heart damage and death. Accordingly, if patients are having symptoms that could represent a myocardial infarction, they should always seek immediate medical attention by dialing 911.
Risk Factors
Myocardial infarctions result from coronary artery disease (CAD). Thus, risk factors for the development of CAD are also risk factors for myocardial infarctions:
- Smoking
- Having high cholesterol levels
- Not exercising regularly
- Having, or high blood pressure
- Eating a diet high in saturated fat and cholesterol
- Having diabetes mellitus
- Being more than 30 percent over one's ideal weight
- Using stimulant or recreational drugs, such as cocaine or amphetamines
- Having family members (especially parents or siblings) who have had coronary artery disease (CAD), myocardial infarctions, or strokes
The common cold
(also known as
nasopharyngitis,
rhinopharyngitis,
acute coryza, or
a cold) is a viral
infectious disease of the upper
respiratory system which affects primarily the nose. Symptoms include a
cough,
sore throat,
runny nose, and
fever which usually resolve in seven to ten days, with some symptoms lasting up to three weeks. Well over 200 viruses are implicated in the cause of the common cold; the
rhinoviruses are the most common.
Upper respiratory tract infections are loosely divided by the areas they affect, with the common cold primarily affecting the nose, the throat (
pharyngitis), and the sinuses (
sinusitis). Symptoms are mostly due to the body's
immune response to the infection rather than to tissue destruction by the viruses themselves. The primary method of prevention is by
hand washing with some evidence to support the effectiveness of wearing face masks.
No cure for the common cold exists, but the symptoms can be treated. It is the most frequent infectious disease in humans with the average adult contracting two to three colds a year and the average child contracting between six and twelve. These infections have been with humanity since antiquity.
ஆஸ்துமா நோய்க்கான காரணங்கள் என்ன?
நோய்க்கான காரணத்தைப் பொருத்து ஆஸ்துமாவை இரண்டாகப் பிக்கிறார்கள்.
Allergic Asthma எனும் முதல் வகையினருக்குக் காரணம் ஒவ்வாமை. பாரம்பயமாக நோய் வருதல், மூக்கடைப்பு, தோல் அலர்ஜி நோய்கள் போன்ற குறிகுணங்களை இப் பிவினர் பெற்றிருப்பர். ரத்தத்தில் நோய் எதிர்ப்புத் தன்மை கொண்ட அணுக்களுக்கு Ig என்று பெயர். நோய் எதிர்ப்புத் தன்மையைக் கொடுக்க டி, ஏ, எம், ஜி, ஈ என ஐந்து வகையான வெள்ளை அணுக்கள் உள்ளன. இவற்றில் சுவாச மண்டல நோய்களை எதிர்க்கவும் உடலுக்கு ஒத்துக்கொள்ளாத பொருள்களை எதிர்க்கவும் IgE என்ற வகை வெள்ளை அணுக்கள் உள்ளன. ஒவ்வாமைத் தன்மையைக் கொண்ட முதல் வகை ஆஸ்துமா நோயாளிகளுக்கு ரத்தப் பசோதனை செய்யும் நிலையில் IgE வகை ரத்த வெள்ளை அணுக்கள் அதிகமாக இருக்கும்.
இந்த காரணங்கள் எதுவுமே இல்லாமல் IgE -ம் அளவுடன் இருந்து மேல்சுவாச மண்டல அழற்சியைத் தொடர்ந்து இரைப்பு வருவது Idiosyncratic asthma எனும் இரண்டாவது வகை.
முதல் வகை ஆஸ்துமா பெரும்பாலும் இள வயதிலேயே வந்துவிடும். இரண்டாம் வகை ஆஸ்துமா வாலிப வயதையொட்டி துவங்குகிறது.
ஆஸ்துமாவின் முக்கிய அறிகுறி என்ன?
மூக்கடைப்பு, தும்மல் ஆகியவற்றுடன் இருமல் ஆரம்பிக்கும். இருமல் தொடங்கியவுடன் நெஞ்சில் உள்ள சளியைத் துப்புவதற்காக நோயாளி எழுந்திருப்பார். ஆனால் சளி எளிதில் வராது. கொஞ்சம் கஷ்டப்பட்டு சளியைத் துப்பும்போது சளியின் தன்மை ஜவ்வசி கஞ்சி போன்று இருக்கும்; ஒரு சிலருக்கு சேமியா போன்று சிறிதளவு சளி வெளியேறும். கொஞ்சம் தூரம் நடந்தால்கூட இரைப்பு ஏற்படும். இளங்காலைப் பொழுது, இரவில் அதிகம் இரைப்பு இருக்கும். இவை ஆஸ்துமாவின் முக்கிய அறிகுறிகள்.
ஆஸ்துமாவா, சைனுசைட்டீஸô–அறிகுறிகளைக் கொண்டு வித்தியாசப்படுத்தித் தெந்துகொள்வது எப்படி?
கண் எச்சல், தலைவலி, மூக்கடைப்பு, தும்மல் ஆகியவை சைனுசைட்டிஸ் நோயின் முக்கிய அறிகுறிகள். சைனுசைட்டிஸ் நோய் இருந்தால் இரைப்பு இருக்காது. தலைவலி, தலையில் நீர் கோர்த்து கனமாக இருப்பது போன்ற உணர்வு ஆகியவை சைனுசைட்டீஸ் நோயின் முக்கிய அறிகுறிகள். மேலும் மூக்கு, தொண்டை ஆகியவற்றை உள்ளடக்கிய மேல் சுவாசப் பாதை நோய் (Upper Respiratory Tract Disease) என சைனுசைட்டீஸ் அழைக்கப்படுகிறது.
ஆஸ்துமாவின் ஆரம்ப அறிகுறிகள் என்ன?
பொதுவாக எந்த அன்னியப் பொருளையும் உள்ளே அனுமதிக்காமல் வெளியே தள்ளிவிடும் தன்மை நுரையீரலுக்கு உண்டு. இதனால்தான் தும்மல் ஏற்படுகிறது. ஆஸ்துமா நோயின் ஆரம்ப அறிகுறியாக தொடக்கத்தில் நுரையீரல் பாதை லேசாகச் சுருக்கமடைந்து, மூக்கடைப்பு, தும்மல் ஏற்படும். அதிகாலை, இரவில் மூக்கடைப்பு, தும்மல் அதிகமாக இருக்கும். மூக்கடைப்பு, தும்மலுடன் நெஞ்சை இறுக்கிப் பிடித்ததுபோன்ற உணர்வு இருக்கும். ஆரம்பத்தில் ஒரு வாரத்துக்கு இவ்வாறு பிரச்சினை இருக்கும்.
நோய் தீவிரமடையும் நிலையில் இரைப்பு (Wheezing) ஏற்படத் தொடங்கும். நோயாளி தன் காதுகளை இரண்டு கைகளால் மூடிக்கொண்டால் இரைப்பின் ஒலியைக் கேட்க முடியும். அது யாழ் ஒலிபோல இருக்கும்.
Sinusitis is inflammation of the paranasal sinuses, which may be due to infection, allergy, or autoimmune issues. Most cases are due to a viral infection and resolve over the course of 10 days. It is a common condition; for example, in the United States more than 24 million cases occur annually
Tuberculosis,
MTB, or TB (short for tubercle
bacillus) is a common, and in many cases lethal,
infectious disease caused by various strains of
mycobacteria, usually
Mycobacterium tuberculosis.
[1] Tuberculosis typically attacks the
lungs but can also affect other parts of the body. It is spread through the air when people who have an active TB infection cough, sneeze, or otherwise transmit their saliva through the air.
[2] Most infections in humans are
asymptomatic and latent, but about one in ten latent infections eventually progresses to active disease which, if left untreated, kills more than 50% of those so infected.
The classic symptoms of active TB infection are a
chronic cough with
blood-tinged sputum,
fever,
night sweats, and
weight loss (the latter giving rise to the formerly prevalent term "consumption"). Infection of other organs causes a wide range of symptoms.
Diagnosis of active TB relies on
radiology (commonly
chest X-rays) as well as microscopic examination and
microbiological culture of body fluids. Diagnosis of latent TB relies on the
tuberculin skin test (TST) and/or blood tests.
Treatment is difficult and requires administration of multiple antibiotics over a long period of time. Social contacts are also screened and treated if necessary.
Antibiotic resistance is a growing problem in
multiple drug-resistant tuberculosis (MDR-TB) infections. Prevention relies on screening programs and
vaccination with the
bacillus Calmette-Guérin vaccine
The word
arthritis comes from the Greek
arthron meaning "joint" and the Latin
itis meaning "inflammation". The plural of arthritis is
arthritides. Arthritis affects the musculoskeletal system, specifically the joints. It is the main cause of disability among people over fifty-five years of age in industrialized countries.
Arthritis is not a single disease - it is a term that covers over 100 medical conditions.
Osteoarthritis (OA) is the most common form of arthritis and generally affects elderly patients. Some forms of arthritis can affect people at a very early age.
What causes arthritis?
In order to better understand what is going on when a person suffers from some form of arthritis, let us look at how a joint works.
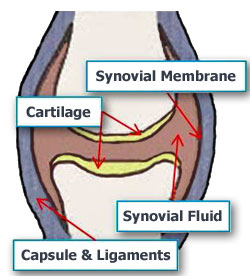
Basically, a joint is where one bone moves on another bone. Ligaments hold the two bones together. The ligaments are like elastic bands, while they keep the bones in place your muscles relax or contract to make the joint move.
Cartilage covers the bone surface to stop the two bones from rubbing directly against each other. The covering of cartilage allows the joint to work smoothly and painlessly.
A capsule surrounds the joint. The space within the joint - the joint cavity - has synovial fluid. Synovial fluid nourishes the joint and the cartilage. The synovial fluid is produced by the synovium (synovial membrane) which lines the joint cavity.
If you have arthritis something goes wrong with the joint(s). What goes wrong depends on what type of arthritis you have. It could be that the cartilage is wearing away, a lack of fluid, autoimmunity (your body attacking itself), infection, or a combination of many factors.
Types of arthritis
There are over 100 types of arthritis. Here is a description of some common ones, together with the causes:
- Osteoarthritis - cartilage loses its elasticity. If the cartilage is stiff it becomes damaged more easily. The cartilage, which acts as a shock absorber, will gradually wear away in some areas. As the cartilage becomes damaged tendons and ligaments become stretched, causing pain. Eventually the bones may rub against each other causing very severe pain.
- Rheumatoid arthritis - this is an inflammatory form of arthritis. The synovial membrane (synovium) is attacked, resulting in swelling and pain. If left untreated the arthritis can lead to deformity. Rheumatoid arthritis is significantly more common in women than men and generally strikes when the patient is aged between 40 and 60. However, children and much older people may also be affected.
- Infectious arthritis (septic arthritic) - an infection in the synovial fluid and tissues of a joint. It is usually caused by bacteria, but could also be caused by fungi or viruses. Bacteria, fungi or viruses may spread through the bloodstream from infected tissue nearby, and infect a joint. Most susceptible people are those who already have some form of arthritis and develop an infection that travels in the bloodstream.
- Juvenile rheumatoid arthritis (JRA) - means arthritis that affects a person aged 16 or less. JRA can be various forms of arthritis; it basically means that a child has it. There are three main types:
1. Pauciarticular JRA, the most common and mildest. The child experiences pain in up to 4 joints.
2. Polyarticular JRA affects more joints and is more severe. As time goes by it tends to get worse.
3. Systemic JRA is the least common. Pain is experienced in many joints. It can spread to organs. This can be the most serious JRA.
What are the signs and symptoms of arthritis?
The symptoms of arthritis depend on the type of arthritis, for example:
- Osteoarthritis - The symptoms develop slowly and get worse as time goes by. There is pain in a joint, either during or after use, or after a period of inactivity. There will be tenderness when pressure is applied to the joint. The joint will be stiff, especially first thing in the morning. The patient may find it harder to use the joint - it loses its flexibility. Some patients experience a grating sensation when they use the joint. Hard lumps, or bone spurs may appear around the joint. In some cases the joint might swell. The most common affected joints are in the hips, hands, knees and spine.
- Rheumatoid arthritis - The patient often finds the same joints in each side of the body are painfully swollen, inflamed, and stiff. The fingers, arms, legs and wrists are most commonly affected. Symptoms are usually worst on waking up in the morning and the stiffness can last for 30 minutes at this time. The joint is tender when touched. Hands may be red and puffy. There may be rheumatoid nodules (bumps of tissue under the skin of the patient's arms). Many patients with rheumatoid arthritis feel tired most of the time. Weight loss is common.
The smaller joints are usually noticeably affected first. Experts say patients with rheumatoid arthritis have problems with several joints at the same time. As the arthritis progresses it spreads from the smaller joints in your hands, wrists, ankles and feet to your elbows, knees, hips, neck, shoulders and jaw.
- Infectious arthritis - The patient has a fever, joint inflammation and swelling. He will feel tenderness and/or a sharp pain. Often these symptoms are linked to an injury or another illness. Most commonly affected areas are the knee, shoulder, elbow, wrist and finger. In the majority of cases, just one joint is affected.
- Juvenile rheumatoid arthritis - The patient is a child. He will experience intermittent fevers which tend to peak in the evening and then suddenly disappear. His appetite will be poor and he will lose weight. There may be blotchy rashes on his arms and legs. Anemia is also common. The child may limp or have a sore wrist, finger, or knee. A joint may suddenly swell and stay larger than it usually is. The child may experience a stiff neck, hips or some other joint.
back pain?
A risk factor is something which increases the likelihood of developing a condition or disease. For example,
obesity significantly raises the risk of developing
diabetes type 2. Therefore, obesity is a risk factor for diabetes type 2. The following factors are linked to a higher risk of developing low back pain:
- A mentally stressful job
- Pregnancy - pregnant women are much more likely to get back pain
- A sedentary lifestyle
- Age - older adults are more susceptible than young adults or children
- Anxiety
- Depression
- Gender - back pain is more common among females than males
- Obesity/overweight
- Smoking
- Strenuous physical exercise (especially if not done properly)
- Strenuous physical work
What are the signs and symptoms of back pain?
A symptom is something the patient feels and reports, while a sign is something other people, such as the doctor detect. For example, pain may be a symptom while a rash may be a sign.
The main symptom of back pain is, as the name suggests, an ache or pain anywhere on the back, and sometimes all the way down to the buttocks and legs. In most cases signs and symptoms clear up on their own within a short period.
If any of the following signs or symptoms accompanies a back pain your should see your doctor:
- Weight loss
- Elevated body temperature (fever)
- Inflammation (swelling) on the back
- Persistent back pain - lying down or resting does not help
- Pain down the legs
- Pain reaches below the knees
- A recent injury, blow or trauma to your back
- Urinary incontinence - you pee unintentionally (even small amounts)
- Difficulty urinating - passing urine is hard
- Fecal incontinence - you lose your bowel control (you poo unintentionally)
- Numbness around the genitals
- Numbness around the anus
- Numbness around the buttocks